Amelogenesis Imperfecta
Amelogenesis imperfecta is a diverse group of hereditary conditions that primarily affect the quality and/or the quantity of dental ENAMEL, resulting in poor development or complete absence of the enamel of the teeth.
This developmental condition is caused by improper differentiation of ameloblasts in the absence of systemic involvement with the phenotypic manifestations of mutant genes influencing different levels of enamel development. Currently, there are four proven candidate genes that play a factor in amelogenesis imperfecta; amelogenin (AMELX), enamelin (ENAM), enamelysin (MMP20), and kallikrein 4 (KLK4). These genes provide instructions for making proteins that are essential for normal tooth development. They are involved in the formation of enamel which is a hard, calcium-rich material that forms the protective outer layer of each tooth. Mutations in any of these genes alter the structure of these proteins or prevent the genes from making any protein at all. As a result, tooth enamel is abnormally thin or soft and may have a yellow or brown colour.
In some cases, the genetic cause of amelogenesis imperfecta has not been identified. Researchers are still working to find mutations in other genes that are responsible for this disorder.

MODES OF MENDELIAN INHERITANCE
1. Autosomal Dominant Inheritance
Can have male to male transmission.
On average, half of the offspring of an affected individual will be affected.
There is a 50% chance for the child of an affected individual to be affected.
Affected males and females have similar clinical presentation.
2.
Autosomal Recessive Inheritance
Unaffected parents will have affected offspring.
On average, one in four offspring of carrier parents will be affected.
More likely to occur when parents are related (consanguineous relationship).
3. X-Linked Recessive Inheritance
Do not have male to male transmission.
All daughters of an affected male are carriers.
Half of the sons born to a carrier female will be affected.
Affected males have more severe manifestations than females.
Females can show no manifestations to severe manifestations due to lyonization.
Females express only one X chromosome per cell with the other X chromosome becoming the bar body. If adequate numbers. of cells express the X chromosome carrying the mutant allele, they will have varying degrees of the enamel defect.
CLINICALLY
The enamel defects are highly variable. People afflicted with amelogenesis imperfecta can suffer from thin and soft enamel and abnormal tooth colours such as yellow, brown or grey. These teeth have a higher risk for dental cavities and are hypersensitive to temperature changes as well as rapid attrition, excessive calculus deposition, and gingival hyperplasia.

On radiographic examination the pulpal outline appears to be normal, and the root morphology is that of normal teeth. The enamel may appear totally absent (lack of enamel opacity) or as thin layer, chiefly over the tips of the cusps & on the interproximal surfaces. In some cases calcification is so much affected that enamel & dentin seem to have the same radio density, making differentiation between the two difficult.
MAIN FORMS OF AMELOGENESIS IMPERFECTA
1. Hypoplastic Form
– Normal or reduced enamel thickness throughout the whole surface, or in isolated areas.
– Enamel pits, grooves, fissures and linear depressions randomly distributed over the entire enamel surface.
- Hard enamel with a normal or slightly yellow-brown color.
– Frequent microfractures of the enamel, and possible attrition.
– Autosomal dominant, X- linked, recessive dominant.

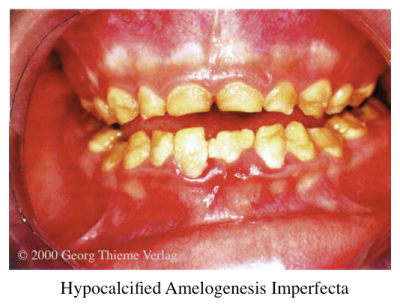
2. Hypocalcified Form:
– Inadequate mineralization. The result is enamel that gets lost a few years after eruption.
- Regular enamel thickness at the time of tooth eruption.
- Soft enamel easily removed.
– Gradual reduction of the thickness resulting from easy attrition.
- Only dentine remains in severe forms of the defect.
- Increased sensitivity in thermal stimuli.
– Yellow-brownish colour of the enamel, with pigment deposition.
– Associated occasionally with anterior skeletal open-bite.
– Autosomal recessive or dominant.
3. Hypomaturation Form
– Adequate deposition of enamel, but the enamel crystal does not mature normally.
– The result is soft pigmented enamel that chips easily.
– Opaque mottled enamel of normal thickness.
– Enamel approaches the radiodensity of dentine.
– Relatively soft enamel with frequent microfractures.
- Mottled brownish-yellow to white appearance.
- Autosomal recessive, dominant or X-linked.

4. Combination Of Hypoplastic And Hypomaturation With Taurodontism
– Hypomaturation-hypoplastic pattern: primary defect is enamel hypomaturation; mottled yellow-white to yellow-brown.
– Hypoplastic-hypomaturation pattern: primary defect is enamel hypoplasia (thin enamel).
– Autosomal dominant.

HISTOLOGICAL FEATURES
Hypoplastic type: disturbance in the differentiation or viability of ameloblasts.
Hypocalcification type: defects of matrix structure and of mineral deposition.
Hypomaturation type: alteration in enamel rod & rod sheath structures.
Since amelogenesis imperfecta carries a high morbidity, including tooth sensitivity, poor esthetics, dental caries, anterior open bite, advanced dental age and/or failure of dental eruption, pre-eruptive tooth resorption, gingival inflammation, and loss of occlusal vertical dimension, the treatment and prognosis are highly variable and relate to the severity of the enamel involvement.
Treatments range from preventive care using sealants and bonding for esthetics to extensive removable and fixed prosthetic reconstruction.
dentodontics.com has potential, you can make your site go viral
easily using one tricky method. Just search in google:
Kelashy’s Method To Go Viral
LikeLike